

What are ABO and Rh blood group systems and how do they affect transfusion
Blood is a specialised connective tissue that circulates throughout the body, transporting oxygen, nutrients, hormones, and waste products. In a healthy individual, about 5 litres of blood flows through blood vessels, maintaining vital functions. The major components of blood include red blood cells (RBCs or erythrocytes), white blood cells (leukocytes), platelets (thrombocytes), and plasma.
Every person’s blood contains specific antigens on the surface of their red blood cells and antibodies in the plasma. These antigens and antibodies form the basis for different ABO blood group system classifications and the Rh system. This classification is crucial for blood transfusion and understanding blood groups and their characteristics.
ABO Blood Group System
The ABO system was discovered by Karl Landsteiner in 1900, for which he later received the Nobel Prize. He observed that mixing blood from different individuals could lead to clumping (agglutination), caused by the interaction of antigens on red blood cells with antibodies in the plasma.
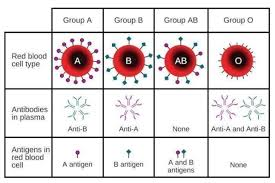
The ABO group is determined by the presence or absence of two key antigens on the surface of RBCs, called antigen A and antigen B:
Group A: Has antigen A on RBCs and antibody B in plasma.
Group B: Has antigen B on RBCs and antibody A in plasma.
Group AB: Has both antigens A and B on RBCs, and no anti-A or anti-B antibodies in plasma.
Group O: Has no antigens (neither A nor B) on RBCs but both anti-A and anti-B antibodies in plasma.
The ABO system is vital when administering blood transfusions. A mismatch can result in red blood cells clumping, leading to serious complications. Here is a quick compatibility guide:
Group A: Can receive blood from A and O groups.
Group B: Can receive blood from B and O groups.
Group AB: Can receive blood from A, B, AB, and O groups (universal recipient).
Group O: Can donate blood to all other ABO groups (universal donor), but can only receive from O.
Rh Blood Group System
In addition to ABO grouping, the Rh system plays a major role in determining if a person’s blood is Rh-positive (Rh⁺) or Rh-negative (Rh⁻). The key antigen in the Rh system is the D antigen.
Rh-positive (Rh⁺): RBCs have the Rh (D) antigen on the surface.
Rh-negative (Rh⁻): RBCs do not have the Rh (D) antigen, but the plasma may develop Rh antibodies upon exposure to Rh-positive blood.
An Rh⁻ individual receiving blood from an Rh⁺ donor (or vice versa) can develop immune reactions if not managed properly. This is especially significant in pregnancy, where an Rh⁻ mother carrying an Rh⁺ foetus may develop antibodies against the foetal RBCs.
Significance of Blood Grouping
Safe Blood Transfusion: Matching ABO and Rh blood groups prevents harmful transfusion reactions.
Organ Transplantation: Correct blood group compatibility reduces rejection risks.
Maternal-Foetal Health: Monitoring Rh compatibility is crucial during pregnancy.
Unique Blood Group Facts
Most Common Blood Type: In many populations worldwide, O positive blood type is considered the most common blood type.
Rarest Blood Type: Commonly, AB negative is cited as the rarest blood type among the ABO-Rh combinations. However, there is also a rare phenotype called the Bombay phenotype (hh), which lacks the precursor antigen for A and B, making it extremely rare in certain parts of the world.
Which is the Strongest Blood Group? There is no official “strongest” group. However, O negative is often called the universal donor because it can be donated to nearly all ABO-Rh groups.
A Positive Blood Type: This is also fairly common in many populations, making it compatible with A positive and AB positive recipients.
Quick Quiz on Blood Groups
Question: Which scientist discovered the ABO blood group system?
Answer: Karl LandsteinerQuestion: Which blood group is known as the universal donor?
Answer: Group O negativeQuestion: Which blood group is known as the universal recipient?
Answer: Group AB positiveQuestion: Which is often cited as the rarest blood type in the ABO-Rh system?
Answer: AB negativeQuestion: Name one important antigen in the Rh system apart from D.
Answer: The C or E antigen
Related Topic Links


FAQs on Blood Groups in Humans and Their Importance
1. What are blood groups?
Blood groups are classifications of human blood based on the presence or absence of specific antigens on the surface of red blood cells (RBCs). These antigens are inherited and determine compatibility during blood transfusion. The two most important blood group systems are:
- ABO blood group system – based on A and B antigens
- Rh blood group system – based on the presence or absence of the Rh factor (D antigen)
2. What are the different types of blood groups in the ABO system?
The ABO blood group system consists of four main blood types: A, B, AB, and O. These types are determined by the antigens present on RBCs:
- Group A – A antigen present; anti-B antibodies in plasma
- Group B – B antigen present; anti-A antibodies in plasma
- Group AB – Both A and B antigens present; no anti-A or anti-B antibodies
- Group O – No A or B antigens; both anti-A and anti-B antibodies present
3. What is the Rh factor in blood groups?
The Rh factor is a protein antigen (D antigen) present on the surface of red blood cells that determines whether a person is Rh-positive or Rh-negative. If the D antigen is present, the blood type is Rh-positive (Rh+); if absent, it is Rh-negative (Rh−). The Rh factor is especially important in pregnancy and blood transfusions to prevent immune reactions.
4. How are blood groups inherited?
Blood groups are inherited through genes passed from parents according to Mendelian inheritance. The ABO blood group is controlled by three alleles: A, B, and O.
- A and B are codominant
- O is recessive
- Genotype AO → Blood group A
- Genotype AB → Blood group AB
- Genotype OO → Blood group O
5. Why is blood group important for blood transfusion?
Blood group is important for transfusion because incompatible blood types can cause a dangerous agglutination reaction. If a recipient receives mismatched blood:
- Antibodies in the plasma bind to foreign antigens
- Red blood cells clump together (agglutinate)
- This can lead to hemolysis and severe complications
6. Who is the universal donor and universal recipient?
In the ABO and Rh system, O negative (O−) is considered the universal donor, and AB positive (AB+) is the universal recipient. This is because:
- O− blood has no A, B, or Rh antigens, reducing risk of reaction
- AB+ individuals have no anti-A, anti-B, or anti-Rh antibodies
7. What is agglutination in blood grouping?
Agglutination is the clumping of red blood cells when antibodies react with matching antigens on their surface. In blood grouping tests:
- Anti-A serum causes clumping if A antigen is present
- Anti-B serum causes clumping if B antigen is present
8. What is hemolytic disease of the newborn (HDN)?
Hemolytic disease of the newborn (HDN) is a condition where maternal antibodies destroy the fetus’s red blood cells due to Rh incompatibility. It commonly occurs when:
- The mother is Rh-negative
- The fetus is Rh-positive
9. What is the difference between ABO and Rh blood group systems?
The ABO and Rh systems differ based on the type of antigens present on red blood cells. The key differences are:
- ABO system – Based on A and B antigens; plasma contains natural antibodies
- Rh system – Based on D antigen; antibodies form only after exposure
10. How is blood grouping tested in the laboratory?
Blood grouping is tested by mixing a blood sample with specific antisera and observing for agglutination. The procedure includes:
- Adding anti-A serum to one sample
- Adding anti-B serum to another sample
- Adding anti-D (Rh) serum to a third sample










